 Dr Dev Mishra Best Orthopaedic Doctor in Delhi NCR Ghaziabad
Dr Dev Mishra Best Orthopaedic Doctor in Delhi NCR Ghaziabad
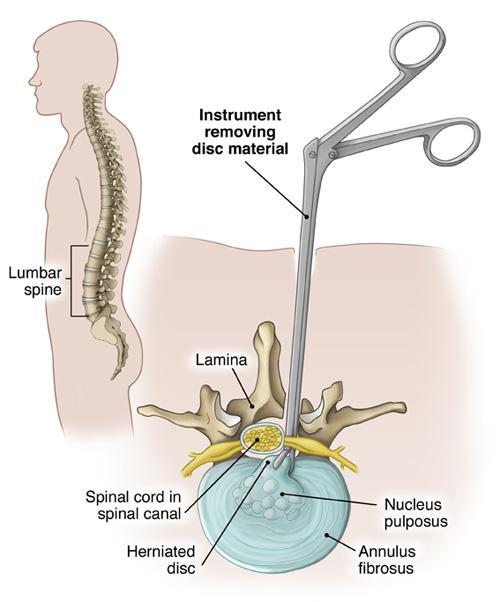
Lumbar Discectomy is performed to removed the herniated portion of the lumbar disc. It has a high success rate, especially in relieving sciatica, caused by the herniated portion of the disc pressing against a nerve.
Dr. Dev Mishra – Senior Orthopaedic Surgeon practicing at Shreya Hospital in Ghaziabad specialize in spine surgery and also have vast experience of doing other Orthopaedic Surgeries.
Types of Lumbar Discectomy
-
Microdiscectomy
Microdiscectomy employs small incision and tissue-preserving techniques to minimize disruption to muscles.
It is generally considered a minimally invasive surgery, as there is minimal disruption of the tissues and structures in the lower back.
The surgical approach is performed through the back, so the patient lies face down on the operating table for the surgery. General anesthesia is used, and the procedure usually takes about one to two hours.
- Microdiscectomy is performed through a small incision – usually 1-2 inches – in the midline of the lower back.
- The back muscles (erector spinae) are lifted off the bony arch (lamina) of the spine and moved to the side. Since these back muscles run vertically, they are held to the side with a retractor during the surgery, and in most cases, they do not need to be cut.
- The surgeon approaches the spine by removing a thick ligamentous membrane over the nerve roots (ligamentum flavum).
- Surgical glasses (loupes) or a microscope allow the surgeon to clearly visualize the surgical field.
- In some cases, a small portion of the inside facet joint is removed both to facilitate access to the nerve root and to relieve any pressure or pinching on the nerve.
- The surgeon may make a small opening in the bony lamina (called a laminotomy) if needed to access the operative site.
- The nerve root is gently moved to the side.
- Surgeon uses small instruments, such as forceps, to remove fragments of herniated disc material under the nerve root.
- Muscles are moved back into place.
- The surgical incision is closed, and surgical strips are placed over the incision to help hold the skin in place to heal.
-
Percutaneous and Endoscopic Lumbar Discectomy
Discectomy is performed under the guidance of fluoroscopy to enable accurate precision.
These two minimally invasive approaches to discectomy are done through a thin tube, or series of tubes, which are inserted into the lower back to provide a corridor of sorts to allow the surgeon to access the offending disc herniation with minimal tissue disruption.
A guide wire is placed within the disc, or near the neuroforamen. Sequential cannulas (thin tubes) are placed over the central guide wire, gradually widening the tube, in order to push apart the surrounding soft tissues to provide an operative corridor.